
Poliovirus: Characteristics, Epidemiology, Serotypes, Mode of transmission, Pathogenesis, Clinical manifestation, laboratory diagnosis, Prevention and control
Characteristics of Poliovirus
- Family: Picornaviridae
- Genus: Enterovirus
- Poliovirus are small, hexagonal, +ssRNA virus
- Symmetry: Icosahedral capsid composed of 60 capsomere
- Each capsomere consists of four viral protein (VP1- VP4)
- Size: 22-30nm
- Shape: spherical
- Genome: positive sense single stranded RNA (+ssRNA).
- The genome is polyadenylated at 3’ end and
- Non-enveloped
Other characteristics of polio virus
- Poliovirus can survive for 4-6 months in cold water.
- It can be inactivated by pasteurization temperature, 0.3% formaldehyde, 0.1M HCL, residual cholorine of (0.3-0.5) ppm
- It is resistant to lipid soluble agents such as Ether, Chloroform, bile and proteolytic enzymes of intestine
- It can survive in faeces for months at 4° C and for years at -20°
Epidemiology: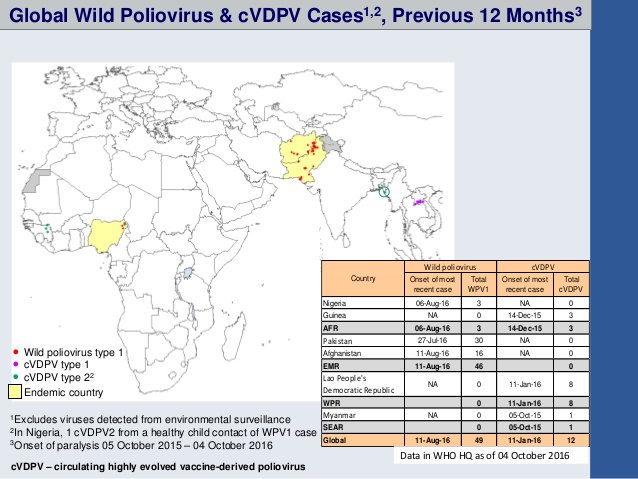
- WHO recorded Polio cases have decreased by over 99% since 1988, from an estimated 350 000 cases in more than 125 endemic countries then, to 37 reported cases in 2016.
- Of the 3 strains of wild poliovirus (type 1, type 2, and type 3), wild poliovirus type 2 was eradicated in 1999 and no case of wild poliovirus type 3 has been found since the last reported case in Nigeria in November 2012.
- Pakistan , Afghanistan and Nigeria are endemic to poliovirus
Serotypes of Poliovirus:
On the basis of neutralization test poliovirus is divided into three serotypes.
- Poliovirus 1: it is most common and virulent type. It is frequent isolated from patients with poliomyelitis and causes epidemics
- poliovirus 2: it is usually associated with endemic infection
- poliovirus 3: it causes occasional endemic infection
Mode of transmission
- Human are only natural host for Poliovirus
- primarily by: Faeco-oral route by Ingestion of virus contaminated food and water
- Droplet infection, inhalation
Pathogenesis
1. Initial multiplication:
- in oropharynx and intestinal epithelium
- Incubation period: 9-12 days
- Virus regularly present in throat and in stool of patient before clinical symptoms
2. Primary viremia:
- Virus enter the lymphatic and blood from oropharynx and intestinal epithelium producing primary viremia
- In most of the case, primary viremia is cleared by host defense. But in children who fail to control primary viremia develop Poliomyelitis.
3. Secondary viremia:
- When primary viremia is not controlled then there is a secondary viremia
- After multiplication in reticuloendothelial syetem, it envades the blood stream again causing major or secondary viremia.
- During secondary viremia, virus crosses the blood-brain barrier and gain access to brain and spinal cord.
- Virus multiply in nerve cell of CNS and damage anterior horn of spinal cord as well as nerve cell of medulla oblongata, pons etc. therefore patients suffer from neurological symptoms
Clinical manifestation:
Few suffer from minor illness, very few suffer from meningitis and less than 1% suffer from major paralytic disease
1. Asymptomatic illness:
- In most of the infection is asymptomatic and self-limiting
2. Abortive poliomyelitis:
- Non-specific symptoms such as headache, fever, sore throat, loss of appetite
- Disease last for 5 days
3. Non paralytic poliomyelitis
- Very few patients suffer from non-paralytic poliomyelitis
- Stiffness of neck
- Pain in back and neck
- Disease last for 2-10 days
4. Paralytic Poliomyelitis:
- Less than 1% patients suffer from major paralytic poliomyelitis
- It damages the motor nerves causing oedema and muscle paralysis
- Malaise
- Anorexia
- Nausea and vomiting
- Sore throat
- Constipation
- Abdominal pain
- Headache and fever
- Flaccid paralysis: motor neuron damage
- Bulbar paralysis: respiratory paralysis
5. Post poliomyelitis muscle atropy:
- Muscle wasting
- Loss of neuromuscular function
- Physically Disabled
6. Death is rare. And if occur it is due to respiratory paralysis
Lab diagnosis:
Specimen: nasal secretion, faecal samples, throat swab, CSF
- Electron Microscopy: virus detection
- Virus isolation: culture on monkey kidney cell line, Human amnion, HeLA, Hep-2, Buffalo green monkey (BGM), MRC-5 cell line
- Antibody detection: ELISA, complement fixation test
- Antigen detection: neutralization test
- Molecular diagnosis: PCR
Treatment: no antiviral drus
Prevention and control:
1. Vaccination
i. Salk’s killed polio vaccine:
- Prepared by Jonas Salk in 1956
- Also known as Inactivated poliovirus vaccine (IPV)
- Prepared by formalin inactivation of poliovirus
- It is injected deep subcutaneous or intramuscular
- Given to child at age of 2 months, 4 months, at school entry age
- Effective against all serotype of poliovirus
ii. Sabin’s vaccine: live attenuated vaccine
- Developed by Albert Sabin in 1962
- Contains live attenuated strain of all serotypes of poliovirus
- It is administered Orally at 2 months of age simultaneously with first DPT
- It is recommended for all children below 5 years
- In endemic countries monovalent oral poliovirus type I vaccine (MOPvI) is introduced to eliminate the last reservoir of poliovirus
2. proper sanitation
3. safe drinking water
References
- http://polioeradication.org/where-we-work/polio-endemic-countries/
- https://www.cdc.gov/polio/about/
- http://polioeradication.org/polio-today/polio-prevention/the-virus/
- http://www.who.int/mediacentre/factsheets/fs114/en/
- http://www.who.int/biologicals/areas/vaccines/poliomyelitis/en/